Lyme disease is the most common infection following an insect bite in the US: the Centers for Disease Control estimates that 300,000 Americans contract Lyme disease each year, calling it “a major US public health problem”. While it is easy enough to treat if caught early, we are still getting to grips with lifelong health problems that can stem from not catching it in time (see “Do I have Lyme disease?“).
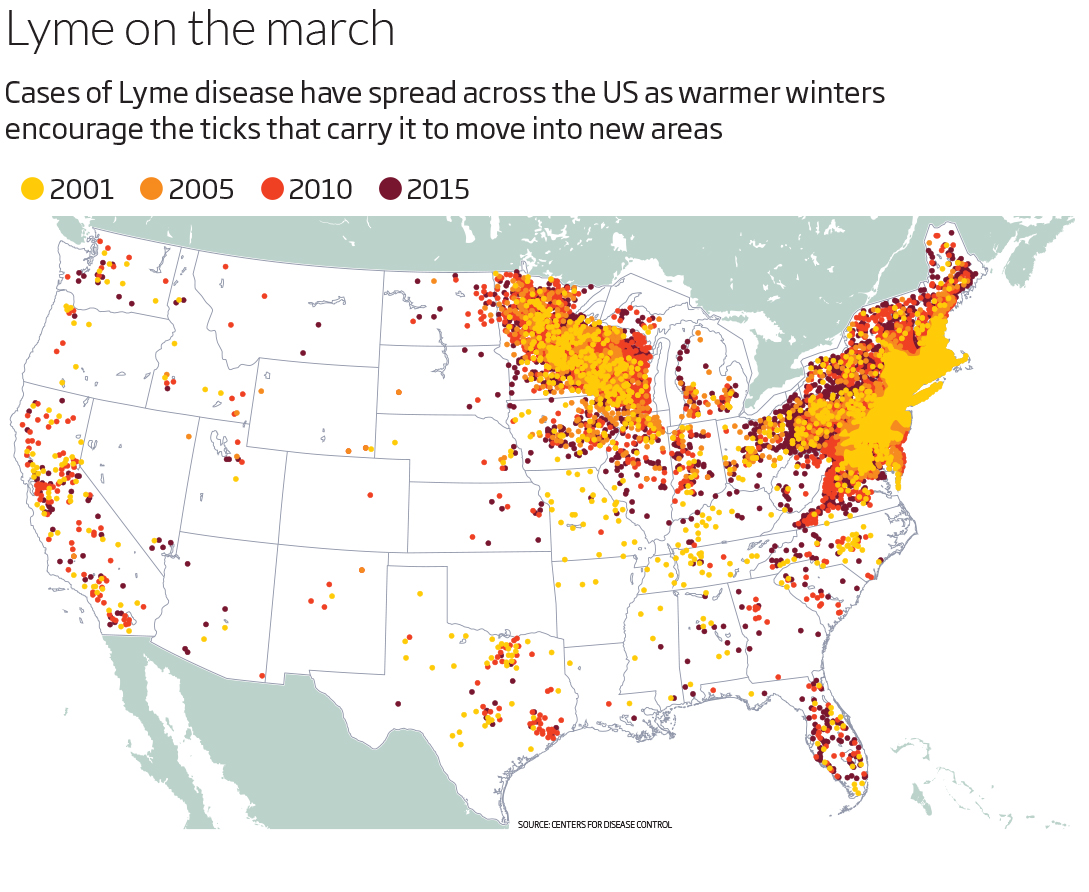
This is less of a problem when Lyme is confined to a few small areas of the US, but thanks in part to warmer winters, the disease is spreading beyond its usual territory, extending across the US (see map) and into Europe and forested areas of Asia. In Europe in particular, confirmed cases have been steadily rising for 30 years – today, the World Health Organization estimates that 65,000 people get Lyme disease each year in the region. In the UK, 2000 to 3000 cases are diagnosed each year, up tenfold from 2001, estimates the UK’s National Health Service.Gut reaction
Once on board, the feast begins. Just one mouse can carry hundreds of immature ticks in their post-larval nymph stage. This is where the problems for us start. Mouse blood carries the Lyme-causing bacterium Borrelia burgdorferi, which passes to a tick’s gut as it feeds. The tick itself is unharmed, but each time it latches onto a new host to feed, the bacteria can move from its gut to the blood – including that of any human passers-by. “We predict the mice population based on the acorns and we predict infected nymph ticks with the mice numbers. Each step has a one year lag,” Ostfeld says. Ostfeld published his discovery of this chain of causation in 2006. Last year, researchers in Poland found the same trend there, with the same implications. “Last year we had a lot of oak acorns, so we might expect 2018 will pose a high risk of Lyme,” says Jakub Szymkowiak at Adam Mickiewicz University in Poznan, Poland. Those who live in traditional Lyme disease zones are well versed in tick awareness – wear long trousers in the woods, check yourself thoroughly afterwards, and more. But this advice will be less familiar in places that used to sit outside Lyme zones – like Poland. “That’s sort of the perfect storm,” says Ostfeld. “The public is unaware, so they’re not looking for it and they don’t get treated.” It’s not obvious when you have been bitten or infected: ticks are the size of a poppy seed, and not everyone gets the classic “bullseye” rash that is supposed to tip you off. The flu-like symptoms that follow are also easy to misdiagnose. And because antibodies to Lyme disease take a few weeks to develop, early tests can miss it. “That’s when you get late-stage, untreated, supremely problematic Lyme disease,” Ostfeld says. The best approach would be to vaccinate people at risk – but there is currently no vaccine. We used to have one, but thanks to anti-vaccination activists, that is no longer the case. In the late 1990s, a race was on to make the first Lyme disease vaccine. By December 1998, the US Food and Drug Administration approved the release of Lymerix, developed by SmithKline Beecham, now GSK. But the company voluntarily withdrew the drug after only four years. This followed a series of lawsuits – including one where recipients claimed Lymerix caused chronic arthritis. Influenced by now-discredited research purporting to show a link between the MMR vaccine and autism, activists raised the question of whether the Lyme disease vaccine could cause arthritis. Media coverage and the anti-Lyme-vaccination groups gave a voice to those who believed their pain was due to the vaccine, and public support for the vaccine declined. “The chronic arthritis was not associated with Lyme,” says Stanley Plotkin, an adviser to pharmaceutical company Sanofi Pasteur. “When you’re dealing with adults, all kinds of things happen to them. They get arthritis, they get strokes, heart attacks. So unless you have a control group, you’re in la-la land.” But there was a control group – the rest of the US population. And when the FDA reviewed the vaccine’s adverse event reports in a retrospective study, they found only 905 reports for 1.4 million doses. Still, the damage was done, and the vaccine was benched. After that, “no one touched it”, says Thomas Lingelbach, CEO at Valneva, a biotech company based in France. Until now: Valneva has a vaccine in early human trials. It will improve on Lymerix, acting against all five strains of the disease instead of just the one most common in the US, and it will be suitable for children. Lingelbach knows the battles his firm will face. “It will be hard to convince anti-vax lobbyists,” he says. That fight is still some way off: any public roll-out is at least six years away. What makes this wait especially galling for some is that there is a vaccine for your pet. “It’s ironic that you can vaccinate your animal and you can’t vaccinate yourself,” Plotkin says. In the animal vaccine, instead of exposing Fido to a weakened version of the antigen to trigger antibodies, it works within the tick, neutralising B. burgdorferi by altering the expression of a protein on the bacterium before it enters the bloodstream. This is how a human version would work. “The underlying scientific principle is not very far away from what it is in the veterinary environment,” says Lingelbach.“It’s ironic that you can vaccinate your animal, but you can’t vaccinate yourself”
Read the entire article on New Scientist.











{kind=link}